Skip to content
Home
About Us
Products
All-ceramics
PFM Restorations
Full Metal Cast
Removable Dentures
Implant Restorations
3D Design Services
Contact Us
Warranty
Eng
Eng
Vi
Eng
Eng
Vi
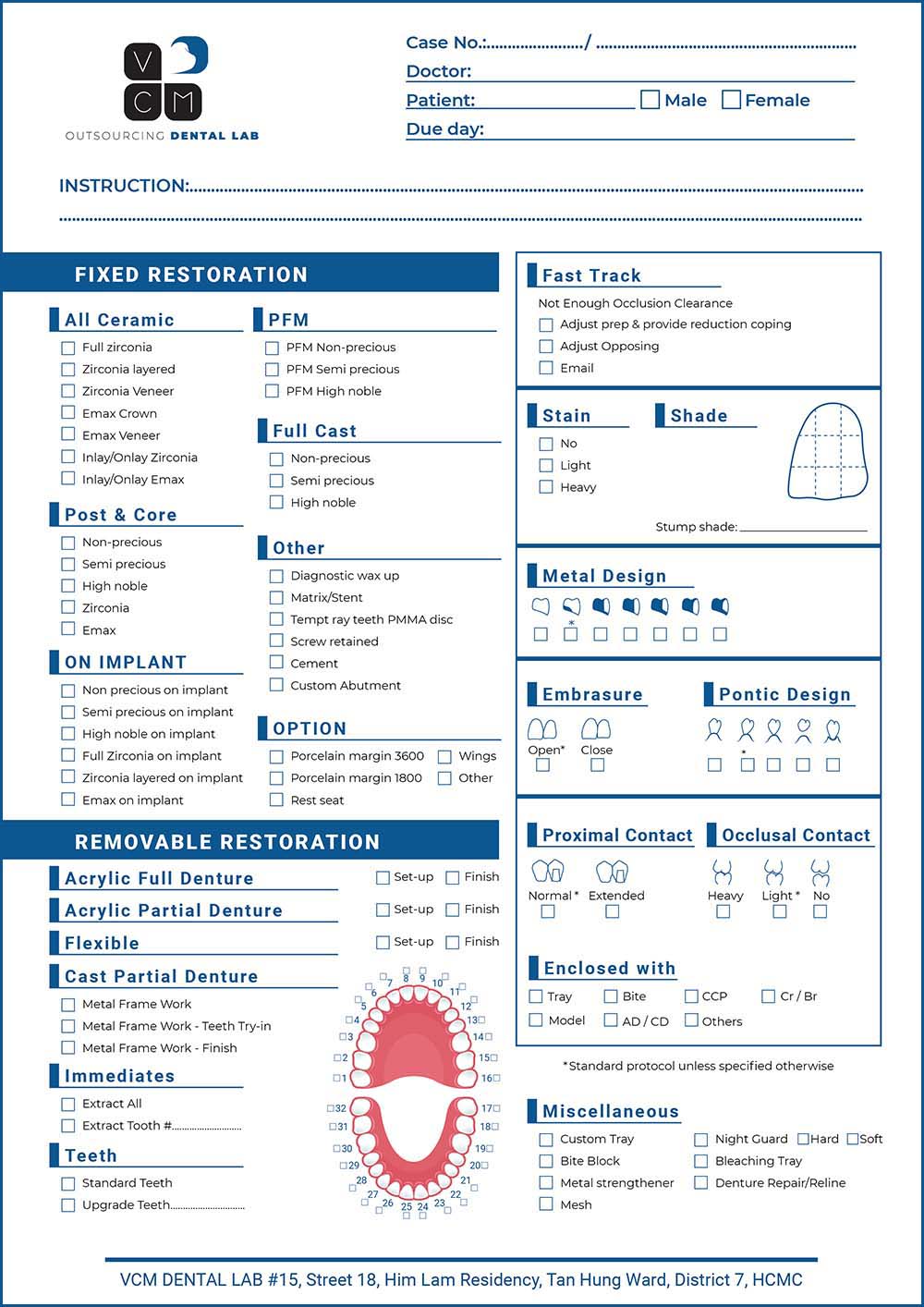
VCM’S RX FORM
Download
SEND US FILES
[contact-form-7 id=”1222″]
Home
About Us
Products
All-ceramics
PFM Restorations
Full Metal Cast
Removable Dentures
Implant Restorations
3D Design Services
Contact Us
Warranty
Login
Username or email address
*
Password
*
Remember me
Log in
Lost your password?

 Vi
Vi